Introduction
How is nutrition support planned in your hospital? How could its organisation be improved? This website has been produced by a multi-professional group under the auspices of BAPEN’s executive and council.
Our website gives you:
- An diagram (look below) to indicate how nutritional services might link within a hospital. Click on each tab below to see the nutritional responsibilities of each. This includes a point by point Powerpoint presentation on hospital food and beverages services accessible from the Catering domain.
- A printable written document. It explains BAPEN’s vision of hospital nutritional organisation and how this derives from national and international reports.
Both the diagram and the written document allow “clickable” direct internet links to the reports on which our ideas are based.
In many countries patients and their relatives retain considerable responsibility for feeding themselves in hospital. While bringing cooked/prepared food in is neither expected nor generally possible in the UK principally because of concerns over food hygiene expressed through the Food Safety Act 1990, it is nonetheless good if the patient and their relatives take a positive approach to improving their nutrition. How?
- Know your weight and height when you go into hospital and think what your usual weight is.
- Make sure someone weighs and measures you when you are admitted to hospital.
- Tell the hospital about your dietary needs and cultural preferences
- Be aware that good nutrition speeds recovery
- Know that illness changes appetite and taste
- If you are not eating enough tell your nurse or doctor
- If you’ve lost weight think about drinks and snacks at home as well as in hospital: milk, cakes biscuits for example. Good nutrition shouldn’t stop when you leave hospital.
- Visit https://www.gov.uk/government/publications/the-eatwell-guide but remember that when you’ve lost a lot of weight “healthy eating” may not be your major priority at first.
- Sometimes people need artificial feeding via a feeding tube placed through their nose into the stomach. Sometimes people need to be fed through a vein. Your hospital should have specialist services organised to supervise these procedures efficiently. Ask about them.
The Hospital Nutrition Steering Committee
Brings together senior managers from many disciplines including nursing, catering, dietetics, pharmacy, medicine & surgery. It may appropriately be chaired by the Head Nurse or a senior figure within the hospital who can provide natural links with Governance and the Board. It may benefit from having sub-committees – for example, Research and Development, Screening, Specialist Services, Catering.
Its remit is across the whole hospital or institution. It:
- Oversees and advises the hospital on all aspects of nutrition, including screening and assessment, catering and food, supplements, enteral and parenteral nutrition – for in-patients and out-patients.
- Scrutinises, develops and co-ordinates hospital nutritional policy in response to external and internal drivers through research and audit.
- Agrees standards for screening, assessment and monitoring; food provision and nutritional support
- Co-ordinates delivery of excellent nutritional support in all units, specialist or general.
- Co-ordinates and monitors appropriate education and training programmes for all staff.
- Liaises with specialist units and if necessary encourages, supports and develops specific needs for nutritional care delivery within them
- Supports at least one multi-professional nutrition support team which includes at least one nutrition nurse specialist
- Oversees the coordinated procurement of supplies relevant to nutrition
- Oversees management of food for staff
- Advises on provision of commercial food outlets on hospital premises
- Is answerable through a governance committee to the hospital board
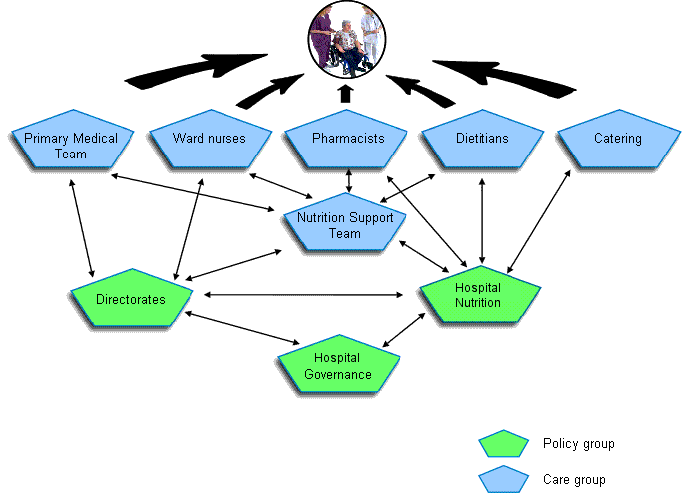
Diagram showing areas of responsibilities for the Hospital Nutrition Steering Committee.

Nutrition Support Team(s) (NST)
Is multi-professional and should include (at least) doctors, nutrition nurse specialist(s), dietitian(s) and pharmacist(s). It should be a role model for multi-professional working. It brings together nutritional experts from medicine/surgery, nursing, dietetics and pharmacy who can co-ordinate the contributions of each of these specialties into coherent nutritional support. It manifestly cannot do all the ward delivery of nutritional care itself, but serves to organise it and enhance it. It becomes particularly involved when there are problems requiring complex artificial nutritional support, especially parenteral nutrition. It may have a specialist role in supporting Home Parenteral Nutrition. The dietitian and pharmacist need to be senior staff and will have a supervisory role within their departments. The team’s operational focus is the safe provision of artificial nutrition but it also has a wider educational remit. It:
- Maintains itself as the principal source of evidence-based information about nutritional assessment and support
- Liaises closely with Nutrition Steering Committee (see above)
- Fosters and provides education, training and research in nutritional screening, assessment, monitoring and nutritional support, for nurses, medical students, doctors, dietitians, pharmacists and managers.
- Develops and audits practical standards of care and organises approaches to nutritional screening, assessment, monitoring and artificial nutrition (eg catheter sepsis rates).
- Is a focus for a multi-professional approach to artificial nutrition and provides co-ordinated medical, pharmaceutical, nursing and dietetic advice on request
- The NST assesses suitability of different feeding routes and advises on alternative treatment options. It particularly directs nutritional care of patients receiving parenteral nutrition or in transition between enteral and parenteral.
- Links to expert capabilities for intravenous catheter and gastrostomy insertion and assists in developing standards for such procedures.
- Provides advice on supplies procurement
- Supports dietitians, particularly in complex enteral feeding cases
- Researches all aspects of artificial nutrition
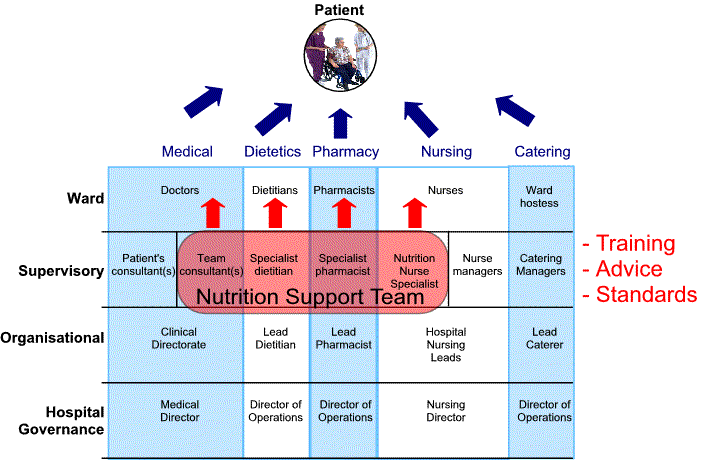
Nutrition Support Team(s) (NST) Diagram showing areas of responsibilities for the Nutrition Support Team
Nutrition Nurse Specialist
- Coordinates Nutrition Support Team with nursing care in general
- Develops safe and practical nursing techniques with respect to nutrition policy through research and audit
- Is a clinical expert in the assessment of nutritional needs and the delivery of treatment.
- Provides advanced technical skills in relation to naso-gastric feeding, Percutaneous Endoscopic Gastrostomy, Radiologically Inserted Gastrostomy and Peripherally Inserted Central Catheters.
- Provides specific training in these skills for nurses, patients and carers.
- Contributes to nutrition education in a broader sense – nursing, medical staff and students
- Advises, with others, on nutrition support policy, linking with the Hospital Nutrition Steering Committee to help develop a coordinated strategy, including issues regarding risk management and ethical decision making
- Links with specialist units to foster good nutritional care.
- Advises on and assists in the procurement of equipment
- Out-patient nutritional support – liaison with community nurses, patients and carers
- Maintains records
- Participates in and often leads audit
- Direct patient advocacy and care – out-patient HEN, HPN. Here the role may come to be seen as that of care manager for nutritional support patients.
Nutrition Support Team Doctor(s)
Nutrition teams need medical involvement, at both consultant and more junior levels. Some patients may be cared for under the consultant’s primary care, though most will usually be under the principal care of another team.
The doctor(s):
- Assess critically the nutritional needs and approach in the context of the patient’s clinical condition and treatment.
- Have a critical awareness of nutrition’s impact on quality of life and clinical outcome
- Have a detailed insight into diagnosis and medical management and how aspects of nutrition relate to these
- Provide a conduit through which Nutrition is linked to the broader hospital medical consensus and teaching.
- Co-ordinate with endoscopy and other gastrostomy-insertion services.
- Maintain links with catheter-insertion services
- Have the expertise to critically appraise a parenteral or enteral nutrition prescription.
- Provide expertise in fluid balance therapy
- Support and conduct nutrition-related audit and research
- Promote the development and maintenance of the Clinical Nutrition Support Team(s) via business planning in hospital and in liaison with Primary Care Commissioning Trusts.
The Nutrition Support Team Dietitian and the Department of Nutrition and Dietetics
The Nutrition Support Team Dietitian needs to be a senior figure within the Department of Dietetics. He/she provides a vital operational and organisational link between the Team and the Department.
The Department:
- Maintains itself as the principal source of evidence-based information on food and nutrition and is an important contributor on nutritional assessment and support
- Supervises and supports dietitians and dietetic assistants
- Provides nutritional advice and expertise in all units of the hospital, including Catering.
- Liaises closely with Nutrition Steering Committee and the Nutrition Support Team(s)
- Participates in education and training
- Assesses diet and nutrition in more detail than a basic screen.
- Provides dietetic advice tailored to individual patient’s needs
- Tailors food and supplements to special dietary/nutritional needs
- Supervises, analyses and interprets dietary records and recalls.
- Prescribes or helps prescribe enteral feeds and supplements, liaising with doctors, nurses and the nutrition support team
- Is “part of the ward” – understands wards and patient problems in order to help solve them
- Liaises with clinical staff including ward nurses, SALT, doctors, occupational therapists and social workers etc
- Advises about enteral feeding techniques
- Advises about parenteral nutrition in liaison with Nutrition Support Team
- Provides community liaison and care (extended roles –links with NNS)
- Provides out patient nutritional care and follow up
The Nutrition Support Team Pharmacist and the Pharmacy
Pharmacy is the home base of the Nutrition Support Team pharmacist and will provide input to nutritional care of patients via ward pharmacists, procurement and via drug advisory services. The NST pharmacist links patient care with pharmacy aseptic services and external, often industrial, suppliers particularly in the context of parenteral nutrition.
- Assists with pre-admission clinic and ward based identification of nutritionally at risk patients.
- Advises on parenteral nutrition composition and compatibilities
- Makes safe additions to standard parenteral feeds or tailor-makes feeds according to the patient’s individual requirements using aseptic technique according to national policy.
- Ensures that parenteral nutritional solutions are compounded appropriately and are suitable for use. This may be via an in-house aseptic unit or outsourced (pharmacy are responsible for audit of external suppliers).
- Appropriately qualified pharmacists may prescribe parenteral feeds, fluids and other necessary therapy.
- Assists with monitoring of parenteral feeding
- Liaises with home care companies for HPN and patients
- Assists in PCT liaison for funding of HPN and high cost drug therapy
- Assists with audit of PN usage and service
- Contributes to nutrition education
- Advises on drug-nutrient and nutrient-nutrient interactions
- Advises on drug delivery via naso-enteric and enterostomy tubes and unblocking parenteral and enteral nutrition delivery systems.
- Purchase and contract for parenteral (and in some cases, enteral) nutrition products and on local formulary content of nutrition-related products.
Catering Services
- Control catering budget and contract: food, beverages and snacks
- Choose and order ingredients
- Develop recipes and menus taking into consideration dietetic advice and patients’ age, culture, religion and medical condition
- Prepare food to approved standards
- Deliver food to wards, patients and staff restaurants
- Serve food to patients at ward level (hostesses)
- Provide snacks
- Maintain and supervise food hygiene at all times
- Consider development of patient restaurants or other novel food delivery/outlets
- Control cost and monitor waste
- Audit and develop service delivery
Please click here to download a Powerpoint presentation on Hospital Food and Catering by Rick Wilson, Kings College Hospital, London.
Links with Hospital Nutrition and NST to adapt hospital policy to directorate use and to develop directorate nutrition policy
- Specialist requirements
- Training and education
- Governance and audit
- Budgets
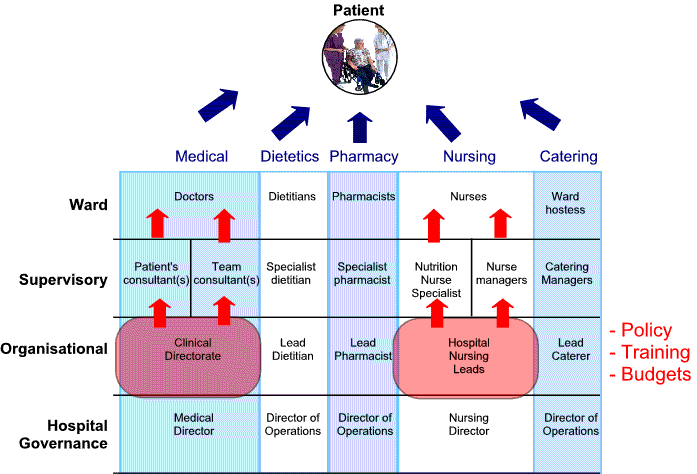
Diagram showing areas of responsibilities for Directorates
Patient’s primary medical team
Must play a co-ordinating role between nutritional and other medical and surgical treatments and ensure that their patients receive excellent nutritional screening, assessment and care.
- Acknowledges the importance of the involvement of all doctors/surgeons in nutritional care as, for example, emphasised by the Royal College of Physicians and PMETB.
- Develops, fosters and encourages an awareness of the benefits of appropriate nutritional management and treatment, before during and after hospital admission, whether surgical or medical.
- Considers the patients’ mental and physical ability to eat, the integrity of gastrointestinal function including motility, digestion and absorption, the metabolism and excretory function in the context of a diagnosis.
- Prescribes treatment, taking into consideration drug nutrient interactions, surgical needs etc
- Takes note of and applies nutritional screening, and assesses and monitors nutrition employing clinical, biochemistry/haematology/microbiology information. Includes documentation of nutrition-related issues in records.
- Decides in liaison with NST, nurses, dietitians etc on the optimal approach to each patient’s nutritional needs and ensures informed consent.
- Liaises with patient and patient’s relatives: provides major source of information to patient and relatives in respect of all aspects of treatment, including nutrition.
- Leads on ethical decisions in conjunction with NST and ward nurses, taking into consideration family/carer views including interpretation of advance directives.
- Includes nutritional aspects of care in plans for discharge and out-patient follow up
- Includes nutrition when liaising with primary healthcare professionals.
Ward Nurses
Are the crucial “final common pathway” of nearly all patient-centred, ward-based care. For Nutrition they should adhere to standards set by Hospital Nutrition Steering Committee which may be adapted locally by Specialist Unit governance. They work in close co-operation with the patient’s principal medical team and the nutrition support team. Together with them they:
- Maintain an ongoing policy towards the nutritional support of patients which has continuity in the context of staff turnover.
- Employ routine nutritional screening including assessment of nutritional risk and the ability of the patient to eat.
- Maximise use of available facilities and options to achieve enjoyable, psychosocially beneficial, nutritionally effective meals and food intake.
- Take responsibility for individual patient’s food intake and co-ordinate a protected mealtimes policy at ward level.
- Help with food choices
- Help with feeding as appropriate
- Monitor/keep records of food intake when necessary
- Are alert to unsafe feeding
- Provide food, and in conjunction with dietitians, supply artificial nutritional supplements
- Provide expert safe delivery and monitoring of artificial nutritional support.
- Deliver enteral and parenteral nutrition skillfully, closely following hospital protocols and guidance
- Monitor enteral and parenteral nutrition – fluid balance, blood/urine glucose, diabetic charts, microbiology
- Prevent (cross) infection.
- Liaise with patient and patient’s relatives
- Employ timely discharge planning and liaise with the community.
Other specialist teams
A major challenge in organising excellent nutrition support is to bring groups together in a common cause to provide the highest quality nutritional care for the patient. It is a major challenge for a clinical team to organise in such a way that it works efficiently with other teams with subtly differing agendas.
Each specialist area in a large hospital may have its own governance, structure and nutrition protocols but these must be in line with overall hospital or institutional policy.
Nutrition Support services link importantly to :
- Radiology (central line insertion, Radiologically Inserted Gastrostomy insertion)
- Endoscopy (Feeding tubes, Percutaneous Endoscopic Gastrostomy, Percutaneous Endoscopic Jejunostomy insertions) will be crucial to practice organisation.
- Speech And Language Therapy will be crucial allies in the care of patients with (potentially) unsafe swallow.
- Nurse led catheter insertion services may link directly or indirectly with nutrition nurse specialists. Liaison over policy development will be vital.
- Infection control team and microbiology: particularly relevant to parenteral nutrition – there needs to be tight coherence in policies.
- Biochemistry services
- Home enteral or parenteral feeding services

Hospital Drivers affecting Nutrition Strategy
| Driver | Rationale |
|---|---|
| Protected meal times | Efficient time for food delivery and assistance, reduced interruptions, increased consumption. Better monitoring |
| Better Hospital food | Menus to reflect and respond to local cultural needs |
| Visiting times | Controlled/ reduced visiting times reduce infection and improve care around meals. Carers (not visitors) stay to help. |
| Patients own food, health & safety | Strict policies /disclaimers. Encourage choice via hospital menu |
| Patient Information | Info on menu completion, meal times, not to bring in own food, dietary advice. |
| Pre admission | Early screening, assessment, and nutritional optimisation |
| Health Care commission Standard 15 (b) | Key core performance standard: all patients on admission to have appropriate and timely screening |
| End of life care | Links with the Liverpool care pathway, ethical dilemmas, good MDT working and decision making: impact quality of life / care and cost, complications and length of stay |
| NICE guidance | Comply or risk register that they are not adopted and why. |
| Infection Control | National Campaign : kitchens, IV’s central lines and urinary catheters etc. MRSA , bacteraemia are reported to a main database. |
| Housekeepers | New housekeeper role not responsible for cleaning i.e. can be involved with nutritional care |
| PEAT | External inspection from a patient perspective |
Core Objectives
These have clinical, humanitarian, environmental and psycho-social dimensions:
- Appropriate nutrient intake for all hospital patients bearing in mind their nutritional status, their length of stay and (changes in) their clinical situation.
- Good food, acceptable to the patient bearing in mind tastes, culture, religion, age, and making allowance for illness.
- A pleasant environment conducive to enjoyment of food and suitable for various states of health and disease, with food able to be delivered to patients flexibly according to their needs in sites such as the ward, ward common room, or a patient restaurant.
- Encouragement of a social component to eating to aid psychological recovery
- Safe and effective artificial feeding
- Pre-admission nutritional support when possible
- Discharge planning and continued community and out-patient nutritional care.
External Recommendations and Reports
ESPEN:
DoH:
BAPEN:
Credits
Chair and editor
Professor Jeremy Powell-Tuck MD FRCP Professor of Clinical Nutrition and Consultant Gastroenterologist, Barts and the London, Queen Mary’s School of Medicine and Dentistry, Chair – Bapen Medical.
Co-chair
Mr Rick Wilson.BSc, SRD. Director of Nutrition and Dietetics, Kings College Hospital.
Committee members:
- Ms Susanne Wood, Formerly Nutrition Nurse Specialist, Barts and the London NHS Trust.
- Mrs Pat Howard, SRD, Director of Nutrition and Dietetics, United Bristol Hospitals Trust, formerly Hon Secretary BAPEN.
- Dr Ian Fellows, DM FRCP Consultant Gastroenterologist, Norfolk and Norwich University Hospital, Honorary Senior Lecturer, University of East Anglia.
- Ms Andrea Cartwright, Senior Nutrition Nurse Specialist, Basildon And Thurrock University Hospitals NHS Foundation Trust, Chair – National Nurses Nutrition Group
- Ms Rebecca White MSc MRPharmS, Lead Pharmacist; Nutrition & Surgery
- John Radcliffe Hospital, Oxford, Chair – BPNG.
Acknowledgement:
We acknowledge the helpful criticisms of many of our colleagues within BAPEN, particularly those of the members of the Education Committee and Council.
